
Till date we seem to be content on two widely accepted theories (1 and 2 below) for myopia progression
1. Genetic Theory: development and progression of myopia is dependent upon genetic factors which could be demonstrated by the more prevalence of myopia in the offspring of parents who both have myopia. Also, genetic factor is determinant to accept the impact of environmental interaction for inducing axial length elongation. This means that if a child is genetically positive for myopia and is exposed to prolonged near work, then chances that his myopia will progress more than similarly genetically negative child with similar duration near work.
2. Environmental Theory: This describes that the progression of myopia is largely dependent upon the hyperopic defocus of the images in the retina. Near work for extended period of time will eventually cause the plane of accommodation to lie behind the reading plane. This lag of accommodation causes the image to be focused behind the retina at a plane conjugate to the accommodative plane. This is called as hyperopic defocus as the eye needs any of two strategies to make the image clear: a) either it should accommodate more, which is not possible because it is due to extensive near work that all the accommodative power has been utilized and lag is seen when optical system surrenders b) It should adjust by gradually shifting the axial length. The latter is most viable option when near work continues for months and years. So, the elongation of axial length is due to the optical blur induced by the hyperopic defocus from prolonged period of near work. One more interesting thing is does eye responds more to central defocus or peripheral defocus. Yes, certainly many researches has shown that eye responds more to the peripheral defocus. That means if peripheral retina is having hyperopic defocus, axial length is going to be increased whereas if peripheral retina suffers from myopic defocus (image in front of retina), axial length is more prone to be shortened. So, the current trends of optical correction that claims to control myopia are based upon this concept. They incorporate positive power in the periphery of the lens and negative power at the center.
3. Not only genetics and environment, but also age of the patient plays a vital role in the myopia progression. The most increase in myopic power occurs from the age of 8 to 15 with approximately 1 Diopter shift in 4 years.
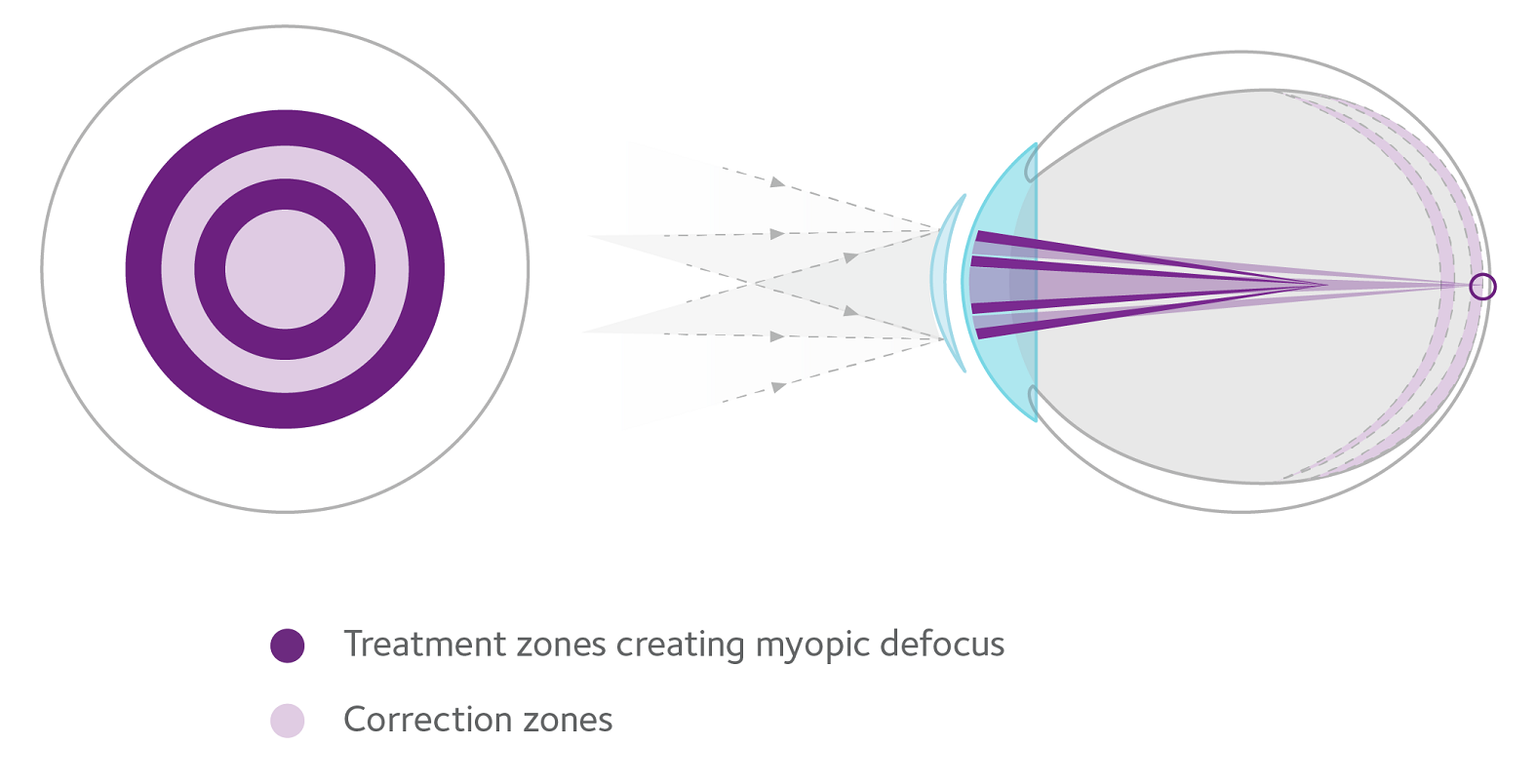
In myopia Control, there are currently four strategies employed: the first one is bifocals or progressive addition lenses, second one is low dose atropine, third one is orthokeratology or corneal reshaping methods and the four one is multifocal contact lenses. In orthokeratology, rigid lenses with reverse geometry are used but in multifocal contact lenses we have MiSight 1 day multifocal soft contact lenses in daily disposable modality by CooperVision. It has two concentric treatment zone with myopic defocus and two correction zone that appropriately corrects the distance myopic error.
Key words: Myopia Progression, Myopia Control, MiSight 1 day, theory of myopia, Short sight, Short sightedness, nearsightedness, near sightedness, low dose atropine, progressive lenses, ortho-k



2 Comments